
![]()
In this section, we dive into how the test results from OralDNA® Labs shaped the personalized treatment plans for Patient A and Patient B. By analyzing both genetic factors and bacterial profiles, we can better understand each patient’s unique risks and challenges. Let’s explore how these insights guided our approach to managing their periodontal disease and improving their overall health
Interpret results for the patient:
Turnaround time is 5 business days with a few days transit. My hygienist and I will sit down and review the results, highlighting areas of concern preparing our patient consultation/review of their results. We utilize EPIC, an electronic health record where patients can access their results once they have been posted.
I start by letting the couple know that I am very happy that we took the test because now we know exactly what we’re up against and can come up with a personalized plan to help manage their periodontal disease.
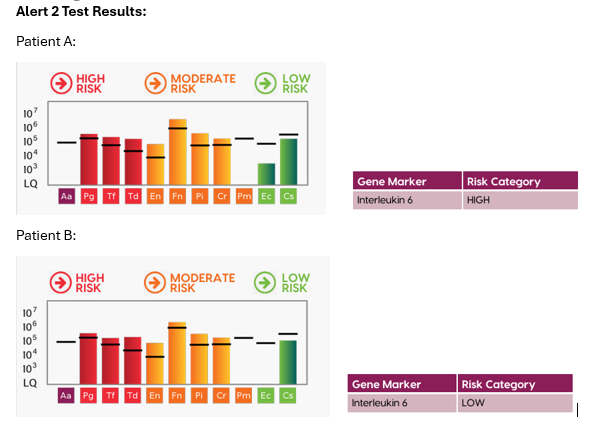
For Patient A (husband), I let him know that from a genetic perspective, he is predisposed to periodontal disease. What that means is someone who is IL-6 high genotype when faced with bad bacteria are more likely to have inflammation with bone loss thus leading to higher risk to develop periodontal disease. Unfortunately, that is nothing that we can change but knowing their genetics helps us know for certain that we need to take a more proactive treatment approach.
Next, I go over his bacterial profile. He has 9 of the 11 different bacteria known to cause periodontal disease and at very high levels. I let him know that there is a perfect storm happening in his body right now because he is already genetically predisposed to inflammation and periodontal breakdown, and now he’s overloaded with all these bad bacteria which is causing gum detachment and bone loss. I let him know that we already are taking steps in the right direction by taking this test and starting the scaling and root planing with the bacterial decontamination laser therapy. That is going to help reduce the overall bacterial levels. Based on test results, I am also going to prescribe the recommended antibiotics for his specific bacterial profile to work in conjunction with his immune system to get those bacteria to a level that is more manageable so that we can reduce clinical signs of infection. I let the patient know that he has some red and orange complex bacteria that are tissue invasive and refractory to treatment so we’re going to need to put him on at home mouth rinses, oral probiotics, and I will need to see him regularly every 3 months for maintenance visits. He’s overwhelmed and somewhat relieved at the same time. I reassure him that I like to think of myself as a “Dental Coach” and at every visit my hygienists and I will track his progress and continue to make recommendations on how he can continue to manage his periodontal disease. He’s thankful because he knew something was off years ago when he started noticing bleeding gums and bad breath and is happy to get treated.
Now it’s Patient B’s turn. I let her know that her IL-6 gene is low. What that means is that compared to someone who is IL-6 high, like her husband, when faced with the same bacteria, her body is less likely to have inflammation and bone loss.
She’s confused and asks, “Well then, why do I have periodontal disease?”
So, I continue to let her know that she has the presence of 8 of the bad bacteria known to cause periodontal disease at very high levels which means her immune system is overloaded right now too. Thankfully, knowing her IL-6 is low, her body was probably better able to resist these bacteria a little longer than her husband’s, but as the bacterial levels rose, then \breakdown started to happen, and the clinical signs started to manifest themselves. I also remind her that when you’re pregnant, your body is even more sensitive to these bacteria and that pregnancy gingivitis and periodontitis are a real thing!
Because she has bacteria above the reference line an antibiotic option is given, however I want her to bring the report to her next OB/GYN appointment so that we can get a medical release from the doctor on next steps. It is especially urgent to get in touch with her medical doctor because Pg, Tf, and Fn put her at risk for pre-term birth, decreased birth weight and even blood infection in the placenta or newborn. We want to make sure that she and baby are safe and healthy.
I transition and lightheartedly joke that I’m going to do a little genetic lesson. Knowing that Dad has IL-6 high means that at the IL-6 gene he has 2 alleles G/G which we know makes him at a higher risk of developing periodontal disease. Mom has IL-6 low, which means her alleles are C/C. Each parent will pass down one of those genes to their child and so the child will have C/G and have an intermediate risk for periodontal disease and other chronic inflammatory diseases. I share that babies are born with sterile mouths without any bacteria and that the bacteria are community acquired, and families tend to share similar bacterial profiles.
I let the couple know that while it’s a lot of information to process, at least we have a clear plan on how to tackle their periodontal disease. I remind them that it’s great that they are both being treated at the same time because couples exchange saliva when they kiss or share utensils or straws. Couples can oftentimes reinfect each other or slow progress because some of those red and orange complex bacteria are transmissible. I encourage the couple to be each other’s accountability partners and stick to their homecare routines and regular 3-month maintenance visits so they can both heal. I remind them that if they can’t do it for each other then I hope they are motivated to do it for their growing baby.
- How Do You Speak Testing? With Bianca Velayo DMD – Part 2 - December 6, 2024
- How Do You Speak Testing? With Bianca Velayo DMD – Part 1 - November 22, 2024
- Interview with Bianca Velayo DMD - April 21, 2023